


The introduction of Mifegymiso (the abortion pill) to Canada in 2017 changed the landscape for abortion services and reproductive healthcare access across the country by enabling tele-medecine and reducing the number of late term abortions.
Although Mifegymiso was legalized in Canada four years ago and is covered by most provincial drug plans, according to health experts, there are still gaps that limit access to abortion throughout Canada.
Within its first year in Canada, provinces adopted the cost of Mifegymiso as a health care system responsibility. Most provinces now cover the drug, which costs approximately $300, apart from Saskatchewan. It remains the only province where the drug is not subsidized.
Greater Access in a Universal pharmacare program
Many organizations across Canada have been calling for a universal pharmacare program to reduce cost and increase access to drugs across Canada including Mifegymiso.
“It would basically increase the accessibility of it for everyone, financially speaking more people would be able to access it,” said Sydney Holmes, co-founder of Defend Choice Ottawa.
Holmes added that a universal pharmacare plan that covered the cost of contraception for women would likely reduce the number of abortions performed per year.
“I think with universal pharmacare you would see a lower rate of abortion in Canada because people would have better access to contraceptives,” she said. “In nations with higher rates of contraceptives they have much lower rates of abortion.”
Dr. Wendy Norman, family physician and public health researcher at the University of British Columbia (UBC) studies abortion trends throughout Canada.
Based on her research, there has been an increase in the use of pill-prescription abortion compared to surgical abortion over the last four years in Canada, and a decrease in late term abortions.
“Emerging data on the uptake of this novel practice indicate more than twice as many practitioners engaged in medical abortion practice within the first year of availability than had provided any abortion service before 2017,” she wrote in a research paper published this year.
Her study of abortion access in Canada also indicated that within a year of Mifegymiso subsidization, nearly a third of all abortions in Ontario and British Columbia were medically induced.
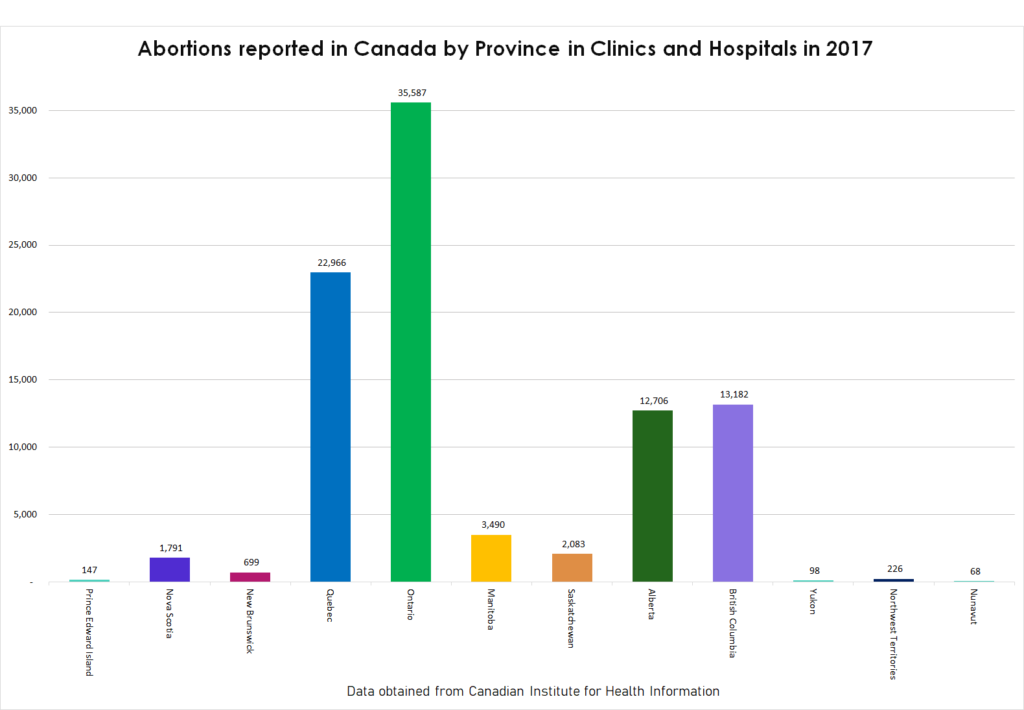
According to the Abortion Rights Coalition of Canada, abortion rates in Ontario have decreased from 39,679 in 2015 to 35,587 in 2017.
Mifegymiso contains mifepristone, a synthetic steroid used to induce abortion. It also contains misoprostol, which is taken as a follow up to mifepristone.
In 2005, the World Health Organization (WHO) added mifepristone and misoprostol, the key components of Mifegymiso, to their list of global essential medicines and health products.
Norman said she would still like to see universal coverage for the pill and contraception to continue eliminating barriers to reproductive healthcare access for women.
“Cost is an access barrier for those who live in rural areas. Despite universal health care, cost is an important and inequitable barrier,” she said.
Norman added that the access to affordable prescriptions will continue to pose barriers for some women until there is universal coverage for all methods.
Currently, coverage for contraceptives in a universal pharmacare plan is unclear, however most provincial pharmacare plans cover a portion of contraceptive medicines and devices.
Moving forward on pharmacare
In 2018, the federal government announced an Advisory Council on the Implementation of National Pharmacare to advise the government on a pharmacare program.
In June 2019, the Council released a report that suggests the first drugs to be provided under the plan should be determined by those deemed essential as indicated on WHO’s Model List of Essential Medicines, and the CLEAN Meds list developed in Toronto.
“The council recommends beginning with a carefully chosen list of essential medicines, available to all Canadians, as the first step towards a fully comprehensive list of drugs,” the authors of the report wrote.
The World Health Organization (WHO) has identified Mifegymiso as clinically, socially, and physically essential for people’s health. It is also included on their list of 450 essential medicines.
“Medical abortion care plays a crucial role in providing access to safe, effective and acceptable abortion care,” their website reads.
The Society of Obstetricians and Gynecologists of Canada (SOGC) supports abortion access for women, while prioritizing the reduction of unplanned pregnancies for women across the country.
“We believe that we can do better in this case and must do what is right to provide sexual health education, free access to contraception, and access to all pregnancy options by removing barriers to access for medical termination of unwanted pregnancies,” SOGC said in a statement.
However, some Canadians disagree with the public funding of contraceptive and abortion services.
Hanna Kepka, Ottawa spokesperson for the Campaign Life Coalition, said she and her organization do not believe in the ethics of abortion.
“Living in our current hook-up culture, unintended pregnancies are an unavoidable consequence,” she said. “We think abstinence is the best solution. Not only as an avoidance of unwanted pregnancy but for moral reasons and emotional ones.”
She added that many birth control options like IUDs, oral contraceptives and implants can have negative side-effects on women’s health. Instead, she suggests abstinence and healthy relationship education in schools as a substitute for contraception and abortion services.
Although some organizations protest the legalization of abortion, all federal candidates in the recent election promised to keep abortion legal.
But there are still barriers that experts say must be addressed to improve abortion access, like education and geography.
Dr. Mei-Ling Wiedmeyer, family physician and women’s health researcher at UBC, said there is only a small number of physicians who provide medical abortion prescriptions in Canada, because some practitioners feel they don’t know enough about the drug.
According to the SOGC, 2,904 health care providers have completed Mifegymiso prescription training.
In Canada, 43,000 family physicians are in practise. According to Norman, family physicians perform the majority of medical and surgical abortions across the country. Despite this, only 500 family doctors were trained by the SOGC to prescribe the pill.
“Some [practitioners] may not feel comfortable because it’s new,” Wiedmeyer said. “Any time you introduce a new process into a clinic now, that can be really challenging.”
She added that there needs to be more resources for doctors with questions about how to prescribe or implement a new prescription process at their clinic to increase the number of prescribers and decrease barriers to access.
“I see people struggling through a very complex system, so for me, I’m in favor,” she said.
According to the Advisory Council’s report, implementation of a universal drug plan could include more programs to inform prescribing practises.
“This strategy would be developed and coordinated at the national level and could then be adapted to support the unique circumstances in different communities across Canada,” the authors of the report wrote.
Wiedmeyer and her team provide resources to health practitioners across Canada that are interested in learning about how to create a prescribing process for the abortion pill in their clinic. But she said there still needs to be more training available for practitioners.
According to Norman, the geographic barrier to accessing reproductive health services takes the highest precedence.
“The most pressing abortion access issue in Canada remains geographic, with significant urban-rural inequities,” Norman said.
One thing Wiedmeyer said she hopes to see with a universal drug plan is that it includes vulnerable populations like migrant women and addresses key access issues for all Canadians, especially geography.
“It’s important for things that are universal–to really be universal,” she said.
Featured image by Paloma Callo.



